In vitro modeling of intestinal absorption plays a pivotal role in advancing preclinical drug development by bridging the gap between laboratory research and clinical application. Predictions of bioavailability derived from cell culture models serve to refine drug design, optimize formulations, and flag potential safety issues. The RepliGut® Planar model is the first intestinal epithelial model that accurately reflects human intestinal contribution to metabolism and transport in a format similar to Caco-2 cells, enabling scientists to further close the gap between in vitro and in vivo bioavailability prediction and reduce late-stage clinical failures.
BCS permeability classification in accordance with the ICH M9 guidance criteria
RepliGut® Planar- Jejunum distinguishes between high and low BCS classification drugs. Correlation between RepliGut® Planar-Jejunum Papp and human absorption. Dotted lines indicate threshold between high and low permeability drugs
RepliGut® Planar- Jejunum distinguishes between high and low BCS classification drugs. Fourteen (14) compounds were tested in accordance with ICH M9 guidance criteria for Papp and compared with known human fraction absorbed (Fa).
High Permeability
Propranolol
Antipyrene
Metoprolol
Desipramine
Theophylline
Carbamazepine
Ketoprofen
Low Permeability
Terbutaline
Atenolol
Enalapril Maleate
Lisinopril
Nadolol
Ranitidine
Furosemide
Correlation of Papp measurements to Caco-2
Comparison of passive permeability between RepliGut® Planar-Jejunum and Caco-2 cells. The apparent permeability of 14 drugs showed a strong correlation, with an R² value of 0.83.
How RepliGut® Planar compares
Ensuring accuracy in intestinal absorption modeling necessitates the presence and functionality of pertinent influx and efflux transporters along with metabolic enzymes. While Caco-2 cells have conventionally served as the benchmark cell culture model for in vitro absorption investigations, their fidelity to native human intestinal tissues is compromised by unregulated proliferation, physiologically inaccurate differentiation processes, and altered expression of drug-related transporters and enzymes, thereby impeding their reliability in mimicking in vivo drug absorption and metabolism.
Feature
Caco-2 Cells
RepliGut® Planar
In Vivo
Human origin
Polarized epithelial monolayer
Multiple cell lineages
Regional specificity maintained
Interindividual variability
Mucus excretion
Phase I and II metabolism
96-well format
Unlike Caco-2 cells, RepliGut® models are comprised of multiple cell lineages found in the in vivo gut, which better reflect in vivo DMPK processes. The cell populations in RepliGut® models are confirmed to be ALP+, MUC2+ and CHGA+ positive and form a polarized monolayer with intact tight junctions.1 Furthermore, RepliGut® Jejunum models express more physiologically relevant levels of several genes encoding phase I and phase II metabolic enzymes reducing the chance of overpredicting bioavailability compared to Caco-2 cells
RepliGut® Models enable you to assess region-specific DMPK endpoints, from more than one donor, for a more thorough vetting of drug candidate bioavailability.
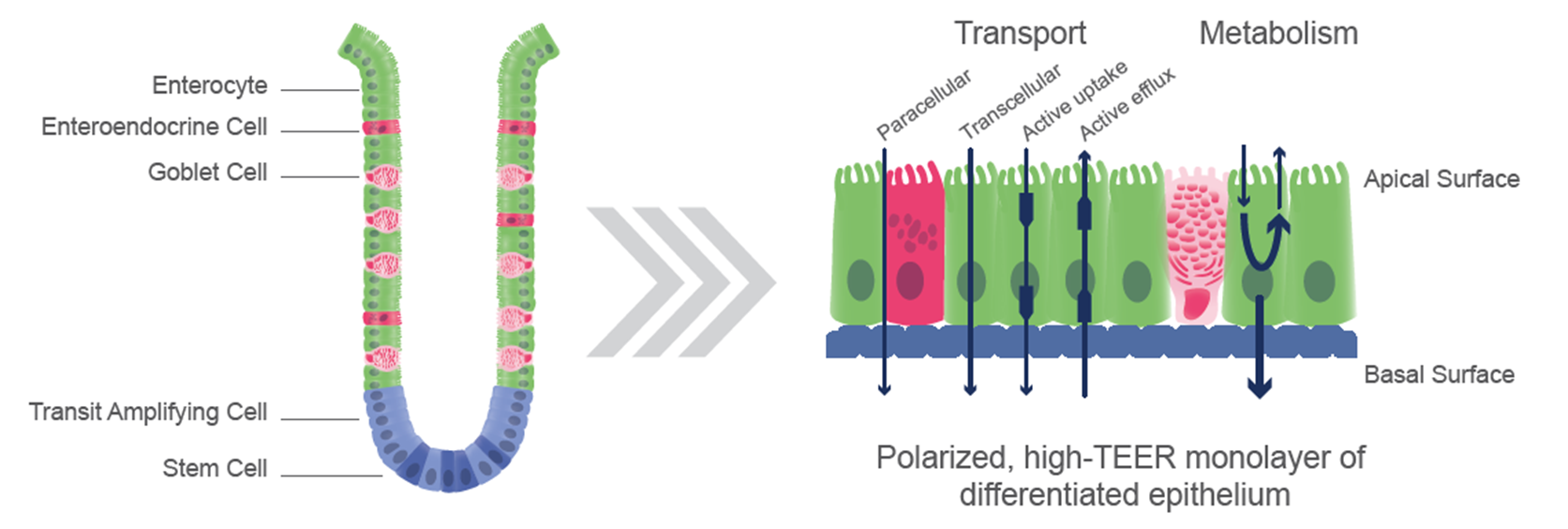
Schematic of RepliGut® Planar. Intestinal crypt-derived stem cells plated onto a semi-permeable membrane differentiate into multiple cell lineages including enterocytes, goblet cells, and enteroendocrine cells. DMPK relevant mechanisms include paracellular and transcellular passive uptake as well as active uptake and efflux. Metabolic processes could include P450, UGT, and CES enzymes.
LC/MS method development with quantitative or qualitative bioanalysis
Comparisons between intestinal regions and donors
Companion barrier integrity monitoring
Apparent permeability (Papp) and efflux ratios
Human jejunum epithelial stem cells are cultured and differentiated on semi-permeable membrane inserts in a 96-well plate to facilitate access to both the apical and basal sides of the cell monolayer. Test compounds are introduced into either compartment to assess their transport in both directions. Accurate mass spectrometry analysis of compound concentrations in each compartment allows for the calculation of permeability (Papp) and efflux ratios. Controls such as atenolol and propranolol, representing low and high permeability respectively, can be included. Additionally, transporter inhibitors can be applied to assess compound interactions with specific transporters. These assays are adaptable to specific research needs.
Typical study design
Cell Culture Timeline
10-11 days
Number of Replicates
Typically 3 wells per treatment
Incubation Time
Up to 120 min
Incubation Buffer
HBSS + 10mM HEPES + 10mM Glucose, pH 7.4
Barrier Integrity Assessment
Automated TEER using EVOM™ Auto (WPI) measured before and after compound incubation
Control Drugs
Atenolol and propranolol
Analysis Method
Accurate mass spectrometry measurement using LC/MS
Data Readout
Papp (apparent permeability coefficient), Efflux ratio, TEER
RepliGut® Planar- Jejunum accurately models passive and active drug transport. (A) Passive and (B) active transport drugs were applied to either the apical or basal compartment and drug concentration was measured in the receiver compartment at 2 hours post exposure. Digoxin and E3S transport were conducted in the presence and absence of P-gp inhibitor, tariquidar, and BCRP inhibitor, Ko143, respectively. Efflux ratios (green) were calculated as the ratio of B→A (pink) to A→B (blue).
Permeability markers tested in RepliGut® Planar-Jejunum
Human jejunum epithelial stem cells are cultured and differentiated on semi-permeable membrane inserts in a 96-well plate to facilitate access to both the apical and basal sides of the cell monolayer. Test compounds are introduced into either compartment to assess their transport in both directions. Accurate mass spectrometry analysis of compound concentrations in each compartment allows for the calculation of permeability (Papp) and efflux ratios. Controls such as atenolol and propranolol, representing low and high permeability respectively, can be included. Additionally, transporter inhibitors can be applied to assess compound interactions with specific transporters. These assays are adaptable to specific research needs.
Drug metabolism and transporter gene expression analysis
Transcriptomic analysis of RepliGut® Planar Systems can provide insights into gut-specific metabolic activity and potential for drug-drug interactions in the GI tract. We offer QuantiGene™ Plex Gene Expression Assays or TaqMan probe RT-PCR to provide targeted gene expression analysis to focus on the impact to your genes of interest. A reference RNAseq data set is available to confirm expression of your gene of interest in RepliGut® Planar- Jejunum.
RNASeq gene expression analysis of RepliGut® Planar-Jejunum vs Caco-2 cells. RepliGut® shows significantly higher expression of critical ADME, Phase I, and Phase II metabolism genes compared to Caco-2 cells. Blue represents low expression. Red represents high expression.
Accurate mass spectrometry method development with quantitative or qualitative bioanalysis
Altis has partnered with BioAgilytix Labs to offer method development and bioanalysis using state of the art LC/MS instrumentation including a high-throughput SCIEX Echo® MS+ coupled to a SCIEX ZenoTOF 7600.
We have isolated epithelial stem cells from multiple intestinal regions obtained from multiple donors, allowing researchers to study colon or small intestine-specific metabolism and transport in demographically diverse backgrounds (e.g. age, sex, blood type). Our cryopreserved biobank enables the ability to work with the same donor as your project progresses or have a variety of donors to evaluate donor differences.
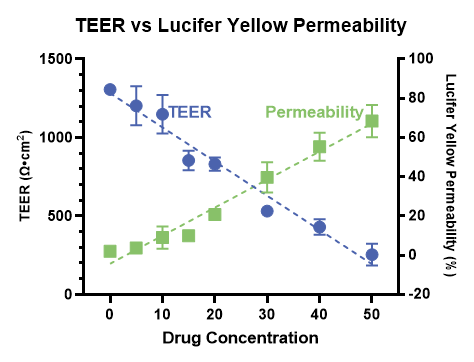
Accurate measurement of paracellular transport requires a consistently tight and intact cell culture barrier throughout the entire experiment. RepliGut® Planar barrier integrity is monitored in real time using Transepithelial Electrical Resistance (TEER). TEER is measured using the high-throughput and automated EVOM™ Auto (WPI) before and after compound incubation to ensure barrier integrity is not compromised.
Relationship between TEER and Lucifer Yellow permeability. The cell culture barrier was disrupted using increasing concentrations of a proinflammatory cytokine. As TEER decreases (blue), indicating a compromised epithelial barrier, there is an increase in Lucifer Yellow permeability (green), reflecting increased paracellular transport of the dye across the epithelial cell monolayer.
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.I agree